
What's in this article?
Primary aldosteronism overview
Aldosterone is the most potent mineralocorticoid produced by the adrenals. It causes Na retention and K loss. In the kidneys, aldosterone causes transfer of Na from the lumen of the distal tubule into the tubular cells in exchange for K and hydrogen. The same effect occurs in salivary glands, sweat glands, cells of the intestinal mucosa, and in exchanges between ICFs and ECFs.
Aldosterone secretion is regulated by the renin-angiotensin system and, to a lesser extent, by ACTH. Renin, a proteolytic enzyme, is stored in the juxtaglomerular cells of the kidneys. Reduction in blood volume and flow in the afferent renal arterioles induces secretion of renin. Renin transforms angiotensinogen from the liver to angiotensin I, which is transformed by ACE to angiotensin II. Angiotensin II causes secretion of aldosterone and, to a much lesser extent, secretion of cortisol and deoxycorticosterone; it also has pressor activity. Na and water retention resulting from increased aldosterone secretion increases the blood volume and reduces renin secretion.
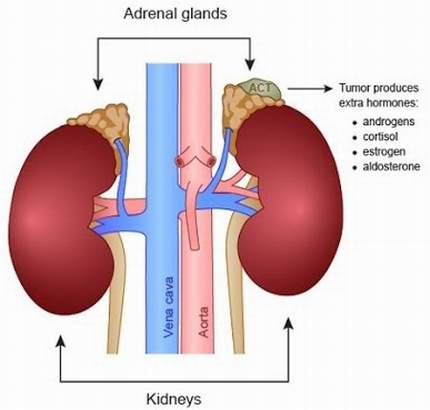
Primary aldosteronism is caused by an adenoma, usually unilateral, of the glomerulosa cells of the adrenal cortex or, more rarely, by adrenal carcinoma or hyperplasia. Adenomas are extremely rare in children, but the syndrome sometimes occurs in childhood adrenal carcinoma or hyperplasia. In adrenal hyperplasia, which is more common among older men, both adrenals are overactive, and no adenoma is present. The clinical picture can also occur with congenital adrenal hyperplasia from deficiency of 11 β-hydroxylase and the dominantly inherited dexamethasone -suppressible hyperaldosteronism. Hyperplasia as a cause of hyperaldosteronism may be more common than previously recognized but remains an infrequent cause in the presence of hypokalemia.
Symptoms of Primary aldosteronism
The most common sign of primary hyperaldosteronism is high blood pressure (hypertension) that does not respond to standard blood pressure medications. Patients with hypertension, especially resistant hypertension (i.e. blood pressure that is difficult to control and that requires multiple medications) should be tested for primary hyperaldosteronism. A low level of potassium in the blood (hypokalemia) is another sign, although patients with normal potassium levels may still have primary hyperaldosteronism. Low acidity of the blood (metabolic alkalosis) also is common. The symptoms of primary hyperaldosteronism are caused by the hypertension and hypokalemia. High blood pressure may cause headache or blurred vision. Low potassium may cause fatigue, muscle cramps, muscle weakness, numbness, or temporary paralysis.
Causes of Primary aldosteronism
Common conditions causing the overproduction of aldosterone include:
- A benign growth in an adrenal gland (aldosterone-producing adenoma) a condition also known as Conn’s syndrome
- Overactivity of both adrenal glands (idiopathic hyperaldosteronism)
In rare cases, primary aldosteronism may be caused by:
- A malignant growth of the outer layer (cortex) of the adrenal gland (adrenal cortical cancer)
- A rare type of primary aldosteronism called glucocorticoid-remediable aldosteronism that runs in families and causes high blood pressure in children and young adults
Complications of Primary aldosteronism
Primary aldosteronism can lead to high blood pressure and low potassium levels. These complications in turn can lead to other problems.
Persistently elevated blood pressure can lead to problems with your heart and kidneys, including:
- Heart attack
- Heart failure
- Left ventricular hypertrophy enlargement of the muscle that makes up the wall of the left ventricle, one of your heart’s pumping chambers
- Stroke
- Kidney disease or kidney failure
- Premature death
High blood pressure caused by primary aldosteronism carries a higher risk of cardiovascular complications than do other types of high blood pressure. This excess risk is due to the high aldosterone levels, which can cause heart and blood vessel damage independent of complications related to high blood pressure.